
GENE EDITING 101: SCIENCE, OVERSIGHT AND OPERATIONAL READINESS (PART 1/2)
The therapeutic application of gene editing has the potential to reshape what “treatment” can look like for patients with certain genetic and other hard-to-treat diseases. For these patients, current options still largely depend on lifelong symptom management with frequent clinic or hospital visits that can pull patients and caregivers away from work, school, and home life. With gene editing, Investigators can change this paradigm by targeting the genetic instructions that give rise to these conditions, supporting interventions that address the root cause, often with a single treatment.
While the promise of gene editing is significant, these kinds of studies can bring complexities that may be new even to experienced clinical sites. Therefore, CROs and sites should plan early for gene editing-specific operational and compliance oversight needs from day one to minimize avoidable activation delays and maximize site readiness.
The Basic Science Behind Gene Editing
At a basic level, gene editing involves making intentional, precise changes to the DNA inside our cells. Depending on the disease and its genetic origin, those changes can be designed to either turn off a gene driving the disease process or correct an “error” in the DNA to restore normal gene-product function.
In practice, most gene-editing approaches use a molecular “GPS” (often a guide RNA) to locate the target DNA sequence, plus an editor (a protein or protein complex) to introduce a planned DNA modification at that site. These components are delivered using viral or nonviral “carrier” systems, each with properties that can affect biodistribution and tissue tropism (where it goes), persistence (how long it stays active), safety profile, and editing efficiency.
One of the best-known platforms is CRISPR (clustered regularly interspaced short palindromic repeats), which uses a guide RNA to direct an enzyme (such as Cas9) to a specific DNA sequence so it can be cut or modified. While CRISPR is well established, it is not always the best fit for every type of genetic change. Other methods, including base editing and prime editing, are being explored for more precise correction of specific variants and small sequence changes.
Regardless of the method used, gene-editing strategies generally fall into two approaches: ex vivo editing and in vivo editing, which differ in where (outside vs. inside the body) and how (cell processing vs. direct delivery) the edit is made.
Ex Vivo Gene Editing: the original clinical workhorse
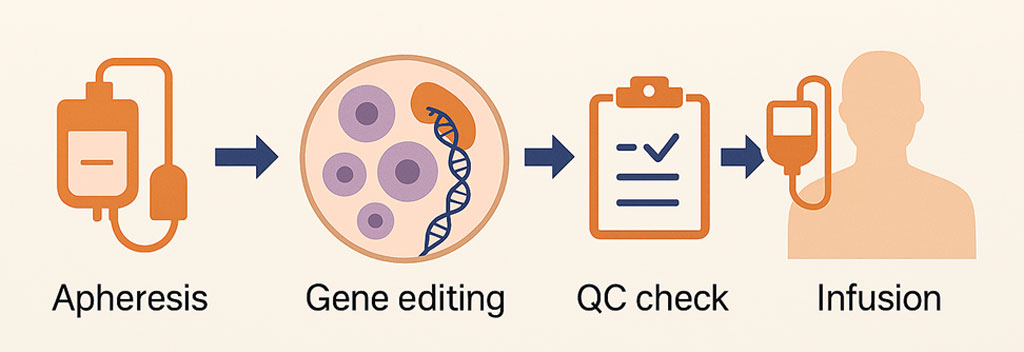
With ex vivo editing, patient-derived cells (for example, hematopoietic stem and progenitor cells or T cells) are collected and modified outside the body, then reinfused into the patient. This approach has been used in oncology, hematology, and immunology, where these cell types can be harvested and returned reliably.
A landmark example of ex vivo editing is Casgevy® (exagamglogene autotemcel), in which blood-forming stem cells are collected and edited to raise fetal hemoglobin. Casgevy® is the first US Food and Drug Administration (FDA)-approved CRISPR-based therapy (first approval: December 8, 2023) and is approved for patients 12 years of age and older with sickle cell disease (SCD) or transfusion-dependent beta thalassemia (TDT).
A major strength of ex vivo workflows is that they offer strong levels of manufacturing control (e.g., quality testing, extensive release criteria, and dose confirmation), which supports consistent product quality and more predictable dosing. However, these workflows are operationally intensive. Beyond the manufacturing challenges, ex vivo programs also require specialized centers with apheresis/cell-collection capability, coordination with cell-processing labs, and infrastructure to manage complex pre- and post-infusion care. Many clinical protocols also use “conditioning” chemotherapy (often lymphodepleting or myeloablative regimens) to create space for the edited cells, which can add risks such as low blood cell counts, infection, bleeding, and, in some cases, hospitalization. For diseases where the desired cells can’t be harvested at scale for ex vivo manufacturing (for example, many solid organs), in vivo editing may be more practical because it delivers the editor directly to the affected tissue.
In Vivo Gene Editing: editing inside the patient
In contrast to ex vivo editing, in vivo editing involves the delivery of the therapeutic editing system directly to the patient, allowing for the key editing step to occur inside the patient after administration. This approach can bypass many of the complex, costly manufacturing steps required for ex vivo gene-edited cells, along with the logistics of cell collection and reinfusion.
Where in vivo gene editing is being applied (high level)
In vivo gene editing is being explored preclinically and clinically across multiple therapeutic areas, often where (1) a clear disease-driving gene is known and (2) efficient delivery to the relevant tissue is feasible. Current activity includes hepatic/metabolic genetic diseases, where liver-directed delivery can reduce or eliminate harmful proteins by targeting genes such as TTR in transthyretin amyloidosis (ATTR) or KLKB1 in hereditary angioedema (HAE). Cardiovascular programs are pursuing one-time strategies intended to durably lower circulating lipids by modifying targets such as PCSK9 (familial hypercholesterolemia/elevated LDL-C) and ANGPTL3 (severe dyslipidemias). Ophthalmology is a strong fit for local delivery, with inherited retinal disease efforts aimed at correcting pathogenic variants in retinal cells, including CEP290-associated Leber congenital amaurosis (LCA) and select monogenic forms of retinitis pigmentosa. Chronic infectious diseases, such as hepatitis B virus (HBV) and human immunodeficiency virus (HIV), are also being targeted by gene editing to disrupt viral persistence or host factors required for infection. Finally, hematology teams are exploring in-body editing to support durable clotting-factor expression or correction for bleeding disorders such as hemophilia A and hemophilia B by targeting F8 and F9 (or by inserting functional factor expression cassettes at liver “safe-harbor” loci such as ALB).
While an active area of exploration, in vivo gene-editing programs are still in their infancy. Most studies are in Phase 1/2, and there are currently no FDA-approved in vivo gene-editing therapies as of the date of this post.
Why In Vivo Gene Editing is So Attractive (and what it must overcome)
In vivo and ex vivo gene editing are complementary approaches, each with distinct clinical and operational constraints. In practice, the choice often comes down to biological fit (which cells/tissues drive the disease), feasibility (which tissues can be reached and safely and efficiently edited), and operational complexity (manufacturing and site requirements).
What makes in vivo editing attractive in practice?
- More “drug-like” administration. Many in vivo products can be delivered by infusion or local injection rather than a transplant-style workflow used for ex vivo approaches.
- Broader tissue reach. It can potentially address diseases in organs where cells can’t be harvested and reinfused at scale (a key limitation for many ex vivo approaches).
- Less patient-specific manufacturing. Compared with ex vivo workflows, in vivo approaches can reduce reliance on multi-week, individualized cell processing and chain-of-identity logistics.
- Scalability and standardization. Dosing can be more standardized than autologous cell products, which may support broader rollout once delivery and safety are established.
- Potentially simpler scheduling and throughput. Removing collection and manufacturing steps can simplify coordination across departments (site-specific requirements still apply) and streamline schedules of activities.
While in vivo editing is attractive for the reasons above (and more), moving the editing process into the body can also increase the risk profile. Researchers must precisely target the right tissues at an effective dose, minimize unintended edits (both off-target and unintended on-target effects), anticipate and manage immune reactions that can affect tolerability and re-dosing, and commit to long-term follow-up and monitoring due to the durability of the changes.
Where Gene Editing is Headed
Gene editing’s next wave of impact will likely hinge on two things: development of more precise and efficient editors and better delivery methods to ensure the editor reaches the right cells, at the right dose, with the right duration, without creating unacceptable safety tradeoffs. As targeting improves, in vivo approaches may reach additional tissues, expanding the range of addressable diseases; in parallel, optimized (or new) editing systems may enable more accurate correction of specific variants, and multiplex editing could help scale allogeneic, off-the-shelf immune cell therapies. Progress will depend on solving persistent challenges, including tissue-specific delivery (and re-dosing), unintended edits, immunogenicity, long-term safety monitoring, and scalable manufacturing and oversight.
What's Next?
With Part 1, we laid down the basic science foundation behind gene editing trials, and it’s the context you need to make smart decisions later. In Part 2, we move from science to execution; starting with how Institutional Review Boards (IRBs) and Institutional Biosafety Committees (IBCs) independently assess gene-editing studies. We’ll break down what each committee is looking for, where submissions tend to get delayed, and how CROs and sites can translate oversight expectations into operational reality, so start-up is faster, cleaner, and more predictable.